Order of triage should not be restricted to order of arrival but should be based on across the room assessment of patients waiting to be triaged1.
Across the room assessment triage.
When performing an across the room assessment the triage nurse uses which senses.
This finding may be a sign of which condition.
A quick visual assessment from across the room will indicate to the triage nurse if someone needs to be bumped to the front of the triage line or rushed to the trauma room for immediate treatment.
Sight and hearing c.
Sight and touch b.
Upon check in the triage nurse makes this assessment based on observation 1 this is a verified and trusted source.
What should the nurse do when a person calls on the telephone for medical advice.
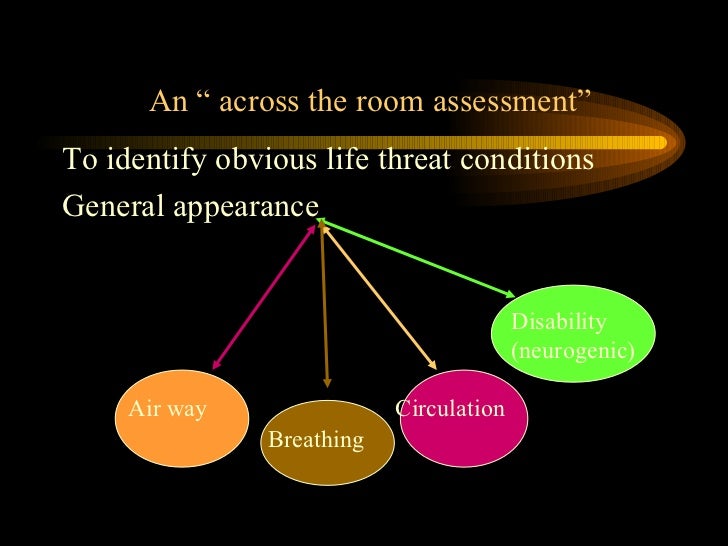
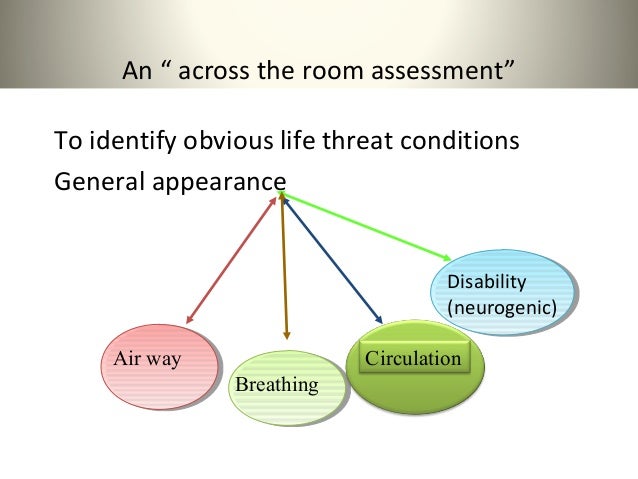
A rapid triage assessment begins with an across the room survey.
A great deal of information can be gathered by visualizing the patient as he or she steps into the waiting room wr.
At anytime during triage if child determined to have an emergent condition triage should be stopped and treatment initiated nursing protocols may be initiated acuity level may change throughout the patient s stay in the emergency department re assessment when patient s in waiting room for 30minutes post triage level 1 red.
The triage nurse notes a fruity smell during an across the room assessment.
7 2 physiological data airway breathing and circulation are the prerequisites of life and their dysfunction are the common denominators of death mcquillan et al.
Observational assessment also known as the across the room look the observational assessment is crucial to determining any necessary initial medical treatment.
It is performed in order to sort injured and ill patients into categories of acuity and prioritization based on the urgency of their medical or psychological needs.
Why do some people have to wait so much longer than others.
Visualizing the patient s appearance as he or she enters the facility is the beginning of the rapid triage assessment.